Hip Dysplasia At Pediatric Orthopedic Specialists
A Healthy Hip Joint Versus One With Hip Dysplasia
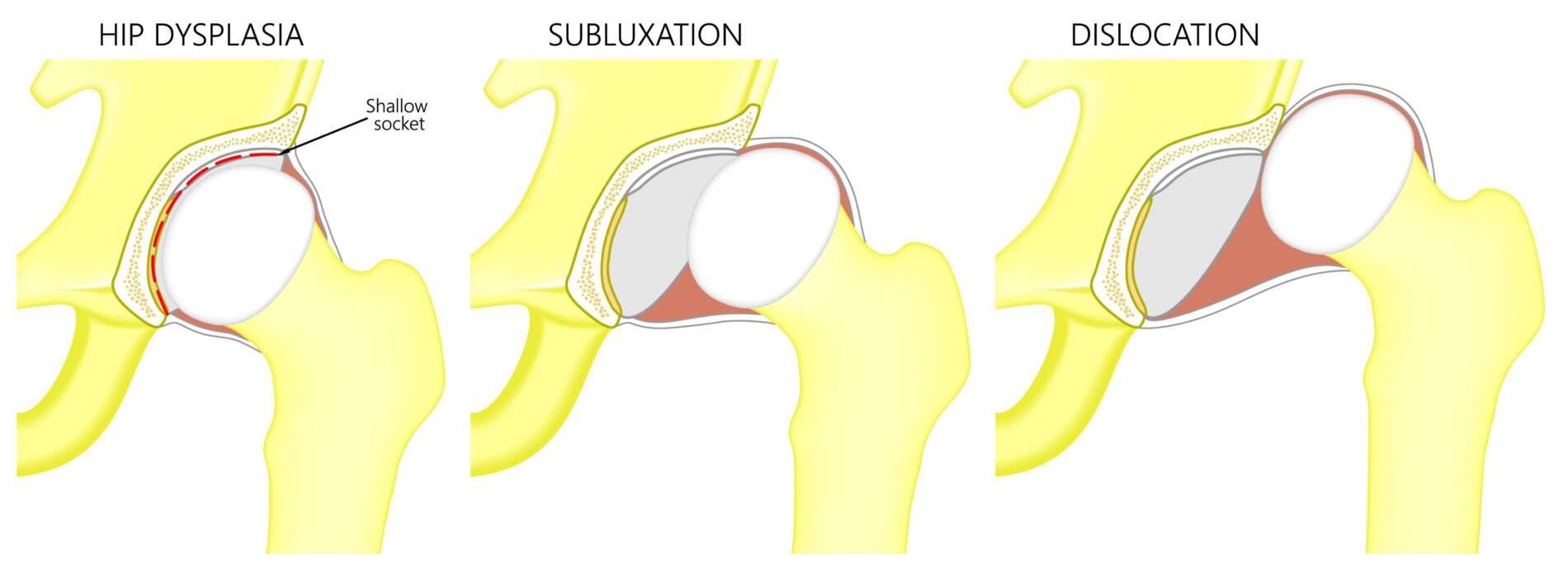
The hip joint is a ball-and-socket joint. The rounded top of the thigh bone fits into the cup shape in the pelvis, allowing a wide range of motion in many directions. A healthy hip joint is very strong and tight, with the ball and socket fitting closely together. In a hip joint with dysplasia, the fit is much looser, and sometimes the joint is partially or fully out of the socket.
This condition can be present from birth or develop in a baby’s first year, and it can affect one hip or both. All babies are checked for hip dysplasia when they are born, then again for every checkup in their first year. It affects 1-2 babies out of every 1000 babies born. It runs in families and is more common in girls and first-born children, as well as babies born breech (bottom-first rather than head-first).
Important Terminology
- Acetabulum: the cup-shaped part of the pelvis that forms the socket part of the hip joint.
- Femoral head: the ball-shaped top end of the femur bone.
- Subluxatable: the femoral head is in place and cannot easily dislocate, but it is loose and can be moved around within the acetabulum.
- Dislocatable: the femoral head is in place but can be pushed out of the socket during a physical exam.
- Dislocated: the femoral head is completely out of the socket.
- Reduced: the hip joint is back in place.
A Hip With Dysplasia
Diagnosis
Treatment for 0-6 Months
We use a Pavlik harness (a soft brace) to hold the hip in place for 1-3 months while the ligaments and joint tissue tighten. This allows the acetabulum to develop normally. Babies wearing these harnesses are still able to move their legs and it doesn’t interfere with diaper changes. We will check the hip’s progress with ultrasounds every 1-2 weeks.
If hip dysplasia persists with Pavlik harness treatment, a stiffer brace may be needed, or we may recommend a closed reduction under anesthesia. This procedure is performed while your baby is safely asleep. The surgeon guides the hip back into place and injects dye to help see when the hip is positioned correctly.
Treatment for 6 Months to 2 Years
By this age, the baby is too big and strong for a Pavlik harness, so a closed reduction under anesthesia followed by a spica case is the typical treatment, sometimes preceded by a few weeks of traction.
If a closed reduction is unsuccessful, open reduction surgery becomes necessary. The surgeon will make an incision to remove the tissue blocking the femoral head from staying in place. The femur bone may need to be shortened in some cases, or the pelvic bone may need to be cut and shifted to deepen the acetabulum. A spica cast is often used during healing after this procedure.
